WO2014167083A1 - Method for predicting the risk of developing a colonic neoplasia - Google Patents
Method for predicting the risk of developing a colonic neoplasia Download PDFInfo
- Publication number
- WO2014167083A1 WO2014167083A1 PCT/EP2014/057343 EP2014057343W WO2014167083A1 WO 2014167083 A1 WO2014167083 A1 WO 2014167083A1 EP 2014057343 W EP2014057343 W EP 2014057343W WO 2014167083 A1 WO2014167083 A1 WO 2014167083A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- fapa
- expression
- patient
- hyperplastic
- fibroblasts
- Prior art date
Links
Classifications
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N33/00—Investigating or analysing materials by specific methods not covered by groups G01N1/00 - G01N31/00
- G01N33/48—Biological material, e.g. blood, urine; Haemocytometers
- G01N33/50—Chemical analysis of biological material, e.g. blood, urine; Testing involving biospecific ligand binding methods; Immunological testing
- G01N33/53—Immunoassay; Biospecific binding assay; Materials therefor
- G01N33/574—Immunoassay; Biospecific binding assay; Materials therefor for cancer
- G01N33/57407—Specifically defined cancers
- G01N33/57419—Specifically defined cancers of colon
-
- G—PHYSICS
- G01—MEASURING; TESTING
- G01N—INVESTIGATING OR ANALYSING MATERIALS BY DETERMINING THEIR CHEMICAL OR PHYSICAL PROPERTIES
- G01N2800/00—Detection or diagnosis of diseases
- G01N2800/56—Staging of a disease; Further complications associated with the disease
Definitions
- the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
- CRC colorectal cancer
- Cancer-associated stroma is a complex medium where a variety of interactions between the tumor and host tissue cells take place. The tumor produces factors that will modify the stroma compartment including the stroma cells. Cancer-Associated Fibroblasts (CAFs), corresponding to fibroblasts present in the tissue stroma that are activated by signals induced by the tumor, represent the main cell population within the stroma.
- CAFs Cancer-Associated Fibroblasts
- FAPa Fibroblast Activation Protein a
- CAFs CAFs and not by the cancer epithelial cells themselves, and represents a marker of the activation of the surrounding fibroblasts by the tumor.
- FAPa could represent an early bio marker for CRC.
- the inventors conducted a 10-year retrospective study on a characterized HP patient cohort (Do et al, 2012) to examine FAPa expression in HP. They show that FAPa expression in colon fibroblasts represents a bio marker allowing predicting the risk of colonic neoplasia in patients presenting with hyperplastic colonic polyps. More precisely, the inventors show in patients, without history of colorectal pathology, presenting initial HP which are considered as non neoplastic (size ⁇ 1 cm and number ⁇ 5), that FAPa expression is significantly higher in HP compared to normal colonic mucosa.
- the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
- the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
- the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
- the invention relates to an in vitro method for determining which patient having hyperplastic polyps will develop a colonic neoplasia (adenomas, adenocarcinomas) after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of an hyperplastic polyp obtained from said patient.
- FAPa for "Fibroblast Activation Protein a” denotes a type II transmembrane serine protease glycoprotein expressed in more than 90% of human epithelial cancers.
- the amino acid sequence of FAPa is described in NCBI database under accession number NP 004451.2 and is also described as the amino acid sequence SEQ ID NO 1.
- the term "colonic neoplasia” or “colonic neoplasm” denotes a tissue whose cells have lost its normal differentiation with abnormalities of nucleus and/or proliferation present in the large intestine (colon, cecum, rectum) including colorectal adenomas (including tubular, villous, tubulovillous and serrated adenomas) and adenocarcinomas.
- hypoplastic polyp denotes a non neoplastic polyp of the large intestine (colon, cecum, rectum) including globlet cell-rich HP, microvesicular HP and mucin poor HP with or without abnormal proliferation [WHO Classification of Tumours of the Digestive System, Fourth Edition and WHO Classification of Tumours, Volume 3 IARC Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D].
- the tissue sample of a hyperplastic polyp may be obtained in the distal or proximal colon, as well as in the cecum or rectum.
- the tissue sample is fibroblasts.
- the fibroblasts are cancer-associated fibroblast (CAFs).
- CAFs cancer-associated fibroblast
- the tissue samples may be obtained from hyperplastic polyps preserved by methods classically used by anatomopathology department, e.g. paraffin embedded or frozen tissues.
- the method is applied on a patient with hyperplastic polyps for which no endoscopic surveillance is recommended neither in the guidelines from the French National Agency for Accreditation and Evaluation in Healthcare, nor by the American College of Gastroenterology (polyp size lower than 1 cm, less than 5 hyperplastic polyps and no family history of hyperplastic polyps).
- determining the level of FAPa expression includes qualitative and/or quantitative detection (measuring levels) with or without reference to a control.
- FAPa expression may be measured for example by RT-PCR or immunohistochemistry performed on the sample.
- the invention relates to a method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia in a patient comprising a step a) consisting of measuring FAPa expression in a sample obtained from said patient.
- the method of the invention further comprises a step of comparing FAPa expression level obtained in step a) to a threshold level.
- control may be a healthy subject, i.e. a subject who does not suffer from any colonic neoplasia.
- the control may also be a subject suffering from colonic neoplasia.
- said control is a healthy subject.
- detecting FAPa expression in sample may be performed by measuring the expression level of FAPa gene.
- the detection comprises contacting the sample with selective reagents such as probes, primers or ligands, and thereby detecting the presence, or measuring the amount, of polypeptides or nucleic acids of interest originally present in the sample.
- Contacting may be performed in any suitable device, such as a plate, microtiter dish, test tube, well, glass, column.
- the contacting is performed on a substrate coated with the reagent, such as a nucleic acid array or a specific ligand array.
- the substrate may be a solid or semi-solid substrate such as any suitable support comprising glass, plastic, nylon, paper, metal, polymers and the like.
- the substrate may be of various forms and sizes, such as a slide, a membrane, a bead, a column, a gel, etc.
- the contacting may be made under any condition suitable for a detectable complex, such as a nucleic acid hybrid or an antibody-antigen complex, to be formed between the reagent and the nucleic acids or polypeptides of the sample.
- the expression level of FAPa gene may be determined by determining the quantity of mRNA of FAPa gene. Such method may be suitable to measure the expression level of FAPa gene in the sample.
- nucleic acid contained in the samples e.g., cell or tissue prepared from the patient
- the extracted mRNA may be then detected by hybridization (e. g., Northern blot analysis).
- the extracted mRNA may be subjected to coupled reverse transcription and amplification, such as reverse transcription and amplification by polymerase chain reaction (RT-PCR), using specific oligonucleotide primers that enable amplification of a region in FAPa gene.
- RT-PCR polymerase chain reaction
- quantitative or semi-quantitative RT-PCR is used. Real-time quantitative or semi-quantitative RT-PCR is particularly advantageous.
- Extracted mRNA may be reverse-transcribed and amplified, after which amplified sequences may be detected by hybridization with a suitable probe or by direct sequencing, or any other appropriate method known in the art.
- LCR ligase chain reaction
- TMA transcription- mediated amplification
- SDA strand displacement amplification
- NASBA nucleic acid sequence based amplification
- Nucleic acids having at least 10 nucleotides and exhibiting sequence complementarity or homology to the mRNA of interest herein find utility as hybridization probes or amplification primers. It is understood that such nucleic acids need not be identical, but are typically at least about 80% identical to the homologous region of comparable size, more preferably at least 85% identical and even more preferably at least 90%, preferably at least 95% identical. In certain embodiments, it will be advantageous to use nucleic acids in combination with appropriate means, such as a detectable label, for detecting hybridization. A wide variety of appropriate indicators are known in the art including, fluorescent, radioactive, enzymatic or other ligands (e. g. avidin/biotin).
- Probes typically comprise single-stranded nucleic acids of between 10 to 1000 nucleotides in length, for instance of between 10 and 800, more preferably of between 15 and 700, typically of between 20 and 500.
- Primers typically are shorter single- stranded nucleic acids, of between 10 to 25 nucleotides in length, designed to perfectly or almost perfectly match a nucleic acid of interest, to be amplified.
- the probes and primers are "specific" to the nucleic acids they hybridize to, i.e. they preferably hybridize under high stringency hybridization conditions (corresponding to the highest melting temperature Tm, e.g., 50 % formamide, 5x or 6x SCC.
- SCC is a 0.15 M NaCl, 0.015 M Na-citrate).
- the method of the invention comprises the steps of providing total RNAs obtained from the sample of the patient, and subjecting the RNAs to amplification and hybridization to specific probes, more particularly by means of a quantitative or semi-quantitative RT-PCR.
- Total RNAs can be easily extracted from the sample.
- the sample may be treated prior to its use, e.g. in order to render nucleic acids available.
- Techniques of cell or protein lysis, concentration or dilution of nucleic acids, are known by the skilled person.
- the expression level of FAPa gene may be measured by DNA microarray analysis.
- DNA microarray or nucleic acid microarray consists of different nucleic acid probes that are chemically attached to a substrate, which can be a microchip, a glass slide or a microsphere-sized bead.
- a microchip may be constituted of polymers, plastics, resins, polysaccharides, silica or silica-based materials, carbon, metals, inorganic glasses, or nitrocellulose.
- Probes comprise nucleic acids such as cDNAs or oligonucleotides that may be about 10 to about 60 base pairs.
- a sample from a test subject optionally first subjected to a reverse transcription, is labelled and contacted with the microarray in hybridization conditions, leading to the formation of complexes between target nucleic acids that are complementary to probe sequences attached to the microarray surface.
- the labelled hybridized complexes are then detected and can be quantified or semi-quantified. Labelling may be achieved by various methods, e.g. by using radioactive or fluorescent labelling. Many variants of the microarray hybridization technology are available to the man skilled in the art (see e.g. the review by Hoheisel, Nature Reviews, Genetics, 2006, 7:200-210).
- Determine the FAPa expression in the tissue sample of a hyperplastic polyp may be performed by determining the expression level of FAPa protein. Any methods that permit to determine the expression of a specific protein in tissues can be used.
- Such methods comprise contacting a tissue sample of a hyperplastic polyp sample with a binding partner capable of selectively interacting with FAPa present in the sample.
- the binding partner may be an antibody polyclonal or monoclonal, an antibody fragment, synthetic antibodies, or other protein- specific agents such as nucleic acid or peptide aptamers.
- the binding partner is a polyclonal or monoclonal antibody.
- a particular method according to the present invention is immunohistochemistry analysis.
- Antibodies specific for FAPa are preferred for this purpose due to specificity and availability.
- Several laboratories have generated and characterized specific FAPa antibodies.
- such antibodies may be easily generated using techniques well-known to those skilled in the art.
- the use of antibodies to identify proteins of interest in the cells of a tissue referred to as immunohistochemistry (IHC), is well established. See for example “Principles and practice of immunoassays" 1991, CP. Price and D.J. Neoman (eds) Stockton Press, N.Y.
- FAPa antibodies may be tagged directly with detectable labels such as enzymes, chromogens or fluorescent probes or indirectly detected with a secondary antibody conjugated with detectable labels.
- detectable labels such as enzymes, chromogens or fluorescent probes or indirectly detected with a secondary antibody conjugated with detectable labels.
- a particular staining method according to the present invention uses a secondary antibody coupled to an amplification system (to intensify staining signal) and enzymatic molecules.
- Such coupled secondary antibodies are commercially available, e.g. from Dako, EnVision system. Counterstaining may be used, e.g. H&E, DAPI, Hoechst.
- the method further comprise a step consisting of comparing the expression level of
- FAPa in the sample with a reference value or threshold value, wherein a difference between said expression level and said reference value is indicative of risk of developing a colonic neoplasia.
- the method further comprise a step consisting of comparing the expression level of FAPa in the sample with a reference value, wherein a difference between said expression level and said reference value is predictive of development of a colonic neoplasia after resection of the HP.
- a “threshold value” or “cut-off value” can be determined experimentally, empirically, or theoretically.
- a threshold value can also be arbitrarily selected based upon the existing experimental and/or clinical conditions, as would be recognized by a person of ordinary skilled in the art.
- the threshold value has to be determined in order to obtained the optimal sensitivity and specificity according to the function of the test (screening, diagnostic, predictive or prognostic) and the remedie/risk balance (clinical consequences of false positive and false negative).
- the optimal sentivity and specificity (and so the threshold value) can be determined using a Receiver Operating Characteristic (ROC) curve based on experimental data.
- ROC Receiver Operating Characteristic
- the person skilled in the art may compare the expression levels of FAPa obtained according to the method of the invention with a defined threshold value.
- the method comprises quantification of the expression of
- FAPa The expression of the FAPa protein is determined by the percentage of fibroblasts cells in the whole hyperplastic polyp that express the FAPa protein.
- the number of positives fibroblasts for FAPa is determined.
- the fibroblasts are cancer-associated fibroblast (CAFs).
- the inventors have established that patients could be at no/low or high risk of colonic neoplastic events when the number of stained fibroblasts was respectively inferior or equal/superior at 9. They also considered 9 stained fibroblasts as a threshold for no/low or a high expression of the protease in HP.
- the inventors also show that patients with no/low expression of FAPa (number of stained fibroblasts inferior at 9) have 91% of neoplasm free-survival at 5 years whereas patients with high expression of FAPa (number of stained fibroblasts equal/superior at 9) have 41% of neoplasm free-survival at 5 years (see figure 3).
- the inventors have established that the association between FAPa staining and neoplasm-free survival is independent from the subject's age, HP localisation and HP size, by performing multivariate analysis (table 2). After adjustment, FAPa expression was still highly significantly associated with adenoma occurrences (p ⁇ 0.022). Taken together, these results show that FAPa staining in HP is a strong independent prognostic factor.
- the present invention also relates to kits for performing the method according to the invention comprising means for determining the level of FAPa expression.
- kits of the invention may comprise an anti- FAPa antibody; and another molecule coupled with a signalling system which binds to said FAPa antibody.
- the antibodies or combination of antibodies are in the form of solutions ready for use.
- the kit comprises containers with the solutions ready for use. Any other forms are encompassed by the present invention and the man skilled in the art can routinely adapt the form to the use in immunohistochemistry.
- the present invention also relates to FAPa as a bio marker for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia.
- the present invention relates to FAPa as a biomarker for determining whether a patient having hyperplastic polyps will develop a colonic neoplasia (adenomas, adenocarcinomas) after resection of said polyp. Predicting method
- the invention in another aspect, relates to a method for predicting the survival time of a patient having hyperplastic polyps comprising the steps consisting of i) determining the level expression of FAPa in a tissue sample from said patient, ii) comparing said level expression with a predetermined reference value and iii) providing a good prognosis of the survival time when the level expression is lower than the predetermined reference value and a poor prognosis of the survival time when the level expression is higher than the predetermined reference value.
- the tissue sample is fibroblasts.
- the fibroblasts are cancer-associated fibroblast (CAFs).
- the number of positives fibroblasts for FAPa is determined.
- tissue samples may be obtained from hyperplastic polyps preserved by methods classically used by anatomopathology department, e.g. paraffin embedded or frozen tissues.
- Determining the level expression of the marker of the invention may be determined by any well known method in the art and described above.
- such methods comprise contacting the tumor tissue sample with at least one selective binding agent capable of selectively interacting with the markers of the invention.
- the selective binding agent may be polyclonal antibody or monoclonal antibody, an antibody fragment, synthetic antibodies, or other protein- specific agents such as nucleic acid or peptide aptamers.
- the selective binding agent binds any of the markers, such as an antibody specific for any of these molecules.
- the antibodies may be tagged directly with detectable labels such as enzymes, chromogens or fluorescent probes or indirectly detected with a secondary antibody conjugated with detectable labels.
- a particular method according to the present invention is immunohistochemistry as explained above. Therapeutic method
- the invention relates to a method of prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention by administrating an antagonist of FAPa.
- the invention relates to a method of prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention by administrating an antagonist of FAPa.
- the invention relates to an antagonist of FAPa for use in a prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention.
- the invention relates to an antagonist of FAPa for use in a prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
- the term "method of prophylactic treatment” denotes a treatment which permits to a patient to not have a colonic neoplasia after resection.
- the "prophylactic treatment” is a preventive treatment.
- the term "antagonist of FAPa” denotes a small organic molecule, an antibody anti-FAPa, an aptamer anti-FAPa, or an inhibitor of the FAPa activity [see for review Kelly et al, 2012, Ellen Pure 2009 or Rui Liu et al, 2012 which are incorporated by reference into the present disclosure].
- the term "inhibitor of the FAPa activity” denotes molecule which is capable of inhibiting the enzymatic activity of FAPa for example, a molecule which is capable of inhibiting the cleavage of c AP or the SPRY2 protein, two substrates of FAPa [for review about FAPa see Kelly et al, 2012].
- said antagonist of FAPa may be a low molecular weight antagonist, e. g. a small organic molecule (natural or not).
- small organic molecule refers to a molecule (natural or not) of a size comparable to those organic molecules generally used in pharmaceuticals.
- Preferred small organic molecules range in size up to about 10000 Da, more preferably up to 5000 Da, more preferably up to 2000 Da and most preferably up to about 1000 Da.
- the antagonist may bind to FAPa and block the binding of other compound on FAPa or the activity of FAPa.
- the peptidyl chloromethyl ketones or the Phe-Arg-(8-amino-3,6-dioxaoctanoic acid)-Gly-[r]-fluoropyrrolidide may be used as inhibitors of FAPa activity [for examples see Kelly et al, 2012].
- Others molecules like boronic acid-based inhibitors such as Val-boroPro, Pro-boroPro, Glu-boroPro and Ala-boroPro may be useful as antagonist [see Kelly et al, 2012 or Rui Liu et al., 2012].
- antagonist of FAPa of the invention may be an anti- FAPa antibody which neutralizes FAPa or an anti- FAPa fragment thereof which neutralizes FAPa.
- Antibodies directed against FAPa can be raised according to known methods by administering the appropriate antigen or epitope to a host animal selected, e.g., from pigs, cows, horses, rabbits, goats, sheep, and mice, among others.
- a host animal selected, e.g., from pigs, cows, horses, rabbits, goats, sheep, and mice, among others.
- Various adjuvants known in the art can be used to enhance antibody production.
- antibodies useful in practicing the invention can be polyclonal, monoclonal antibodies are preferred.
- Monoclonal antibodies against FAPa can be prepared and isolated using any technique that provides for the production of antibody molecules by continuous cell lines in culture.
- Techniques for production and isolation include but are not limited to the hybridoma technique originally described by Kohler and Milstein (1975); the human B-cell hybridoma technique (Cote et al, 1983); and the EBV-hybridoma technique (Cole et al. 1985).
- techniques described for the production of single chain antibodies can be adapted to produce anti-FAPa single chain antibodies.
- FAPa antagonists useful in practicing the present invention also include anti-FAPa antibody fragments including but not limited to F(ab')2 fragments, which can be generated by pepsin digestion of an intact antibody molecule, and Fab fragments, which can be generated by reducing the disulfide bridges of the F(ab')2 fragments.
- Fab and/or scFv expression libraries can be constructed to allow rapid identification of fragments having the desired specificity to FAPa.
- Humanized anti-FAPa antibodies and antibody fragments therefrom can also be prepared according to known techniques.
- “Humanized antibodies” are forms of non-human (e.g., rodent) chimeric antibodies that contain minimal sequence derived from non-human immunoglobulin.
- humanized antibodies are human immunoglobulins (recipient antibody) in which residues from a hypervariable region (CDRs) of the recipient are replaced by residues from a hypervariable region of a non-human species (donor antibody) such as mouse, rat, rabbit or nonhuman primate having the desired specificity, affinity and capacity.
- donor antibody such as mouse, rat, rabbit or nonhuman primate having the desired specificity, affinity and capacity.
- framework region (FR) residues of the human immunoglobulin are replaced by corresponding non-human residues.
- humanized antibodies may comprise residues that are not found in the recipient antibody or in the donor antibody. These modifications are made to further refine antibody performance.
- the humanized antibody will comprise substantially all of at least one, and typically two, variable domains, in which all or substantially all of the hypervariable loops correspond to those of a non-human immunoglobulin and all or substantially all of the FRs are those of a human immunoglobulin sequence.
- the humanized antibody optionally also will comprise at least a portion of an immunoglobulin constant region (Fc), typically that of a human immunoglobulin.
- Fc immunoglobulin constant region
- the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application WO02083171.
- the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application US2002099180.
- the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application WOO 168708.
- the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application DEI 0013286.
- the antibody anti-FAPa according to the invention may be the F19 antibody or his humanized version, the sibrotuzumab, as explained in Kelly et al, 2012 or Rui Liu et al., 2012.
- the antibody anti-FAPa according to the invention may be the FAP5-DM1 antibody as explained in Rui Liu et al, 2012.
- FAPa antagonists may be selected from aptamers.
- Aptamers are a class of molecule that represents an alternative to antibodies in term of molecular recognition.
- Aptamers are oligonucleotide or oligopeptide sequences with the capacity to recognize virtually any class of target molecules with high affinity and specificity.
- Such ligands may be isolated through Systematic Evolution of Ligands by Exponential enrichment (SELEX) of a random sequence library, as described in Tuerk C. and Gold L., 1990.
- the random sequence library is obtainable by combinatorial chemical synthesis of DNA. In this library, each member is a linear oligomer, eventually chemically modified, of a unique sequence.
- Peptide aptamers consists of a conformationally constrained antibody variable region displayed by a platform protein, such as E. coli Thioredoxin A that are selected from combinatorial libraries by two hybrid methods (Colas et al, 1996).
- a peptide like the Melittin or the promelittin may be used to selectively killed FAPa expressing cells [see Kelly et al, 2012].
- Another object of the invention relates to an antagonist of FAPa for use in the prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
- the invention relates to an antagonist of FAPa for use in the prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention.
- Compounds of the invention may be administered in the form of a pharmaceutical composition, as defined below.
- said compound is an antagonist of FAPa.
- a “therapeutically effective amount” is meant a sufficient amount of compound to treat and/or to prevent a colonic neoplasia after resection. It will be understood that the total daily usage of the compounds and compositions of the present invention will be decided by the attending physician within the scope of sound medical judgment.
- the specific therapeutically effective dose level for any particular patient will depend upon a variety of factors including the disorder being treated and the severity of the disorder; activity of the specific compound employed; the specific composition employed, the age, body weight, general health, sex and diet of the patient; the time of administration, route of administration, and rate of excretion of the specific compound employed; the duration of the treatment; drugs used in combination or coincidental with the specific antagonist employed; and like factors well known in the medical arts.
- the daily dosage of the products may be varied over a wide range from 0.01 to 1,000 mg per adult per day.
- the compositions contain 0.01, 0.05, 0.1, 0.5, 1.0, 2.5, 5.0, 10.0, 15.0, 25.0, 50.0, 100, 250 and 500 mg of the active ingredient for the symptomatic adjustment of the dosage to the patient to be treated.
- a medicament typically contains from about 0.01 mg to about 500 mg of the active ingredient, preferably from 1 mg to about 100 mg of the active ingredient.
- An effective amount of the drug is ordinarily supplied at a dosage level from 0.0002 mg/kg to about 20 mg/kg of body weight per day, especially from about 0.001 mg/kg to 7 mg/kg of body weight per day.
- Compounds according to the invention may be used for the preparation of a pharmaceutical composition for the prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
- the present invention also provides a pharmaceutical composition comprising an effective dose of an antagonist of FAPa according to the invention.
- Any therapeutic agent of the invention may be combined with pharmaceutically acceptable excipients, and optionally sustained-release matrices, such as biodegradable polymers, to form therapeutic compositions.
- “Pharmaceutically” or “pharmaceutically acceptable” refers to molecular entities and compositions that do not produce an adverse, allergic or other untoward reaction when administered to a mammal, especially a human, as appropriate.
- a pharmaceutically acceptable carrier or excipient refers to a non-toxic solid, semi-solid or liquid filler, diluent, encapsulating material or formulation auxiliary of any type.
- the form of the pharmaceutical compositions, the route of administration, the dosage and the regimen naturally depend upon the condition to be treated, the severity of the illness, the age, weight, and sex of the patient, etc.
- compositions of the invention can be formulated for a topical, oral, intranasal, parenteral, intraocular, intravenous, intramuscular or subcutaneous administration and the like.
- the pharmaceutical compositions contain vehicles which are pharmaceutically acceptable for a formulation capable of being injected.
- vehicles which are pharmaceutically acceptable for a formulation capable of being injected.
- These may be in particular isotonic, sterile, saline solutions (monosodium or disodium phosphate, sodium, potassium, calcium or magnesium chloride and the like or mixtures of such salts), or dry, especially freeze-dried compositions which upon addition, depending on the case, of sterilized water or physiological saline, permit the constitution of injectable solutions.
- the doses used for the administration can be adapted as a function of various parameters, and in particular as a function of the mode of administration used, of the relevant pathology, or alternatively of the desired duration of treatment.
- compositions include, e.g. tablets or other solids for oral administration; time release capsules; and any other form currently can be used.
- FIGURES
- Figure 1 FAPa-expression in normal, HP, low-grade dysplasia tubular adenoma (TA), high-grade dysplasia TA, and adenocarcinoma
- 'a' threshold corresponding to the number of 9 or more FAPD -stained fibroblasts in HP, had a sensitivity of 81.25% and a specificity of 87.93% that actually represents the optimal sensitivity and specificity couple.
- Se sensitivity
- Spe specificity
- Figure 3 Kaplan-Meier survival estimate based on the number of FAPa expression in HP patients
- Neoplasm-free survival among patients with colonoscopy follow-up according to FAPa expression P-value corresponds to logrank univariate analysis.
- FAPa expression was recorded as “No/low expression” or "high expression” based on the number of stained fibroblasts counted in 20 randomly picked microscope fields at XI 000 magnification.
- the threshold of FAPa expression in HP was determined to be 9 stained fibroblasts, 9 corresponding to the optimal specificity/sensibility couple based on the ROC analysis,
- Neoplam-Free Survival among patients with colonic hyperplastic polyps who had a colonoscopic follow-up was conducted using a Cox model including all variables with a P value ⁇ 0.20 in the univariate analysis.
- the initial Cox model included the age, the size, the localisation of the polyps and FAPa expression.
- Final model was obtained after backward stepwise selection, keeping only the variables with a P value ⁇ 0.05 (i.e. age and FAPa). 95% CI was calculated for all 5-year survival values.
- the FAPa staining has been done on colon tissue sections from 64 patients. 39 patients had colon hyperplastic polyps, 6 had low grade adenomas, 4 presented with high grade adenomas and 5 displayed adenocarcinomas. FAP staining was also examined on normal tissue sections from 10 patients with resected non complicated diverticula. The characteristic of the 39 patients presenting with HP have been previously published (Do et al, 2012). These 39 patients were diagnosed for HP in the Pathology department of Rangueil Hospital in 2000 and 2001.
- FAPa expression was recorded as 'no/low expression' or 'high expression' based on the number of stained fibroblasts counted in twenty randomly chosen microscope fields of the polyp section at XlOOO magnification. For patients with several polyps, the polyp with the wider hyperplastic area was retained for evaluation. Based on the receiver operating characteristic analysis, we found that the optimal specificity/sensibility couple corresponds to a threshold of 9 FAPa-stained fibroblasts. Thus, we established that the overexpression threshold corresponds to a number of stained fibroblasts in hyperplastic polyp equal or higher than 9. The association between FAPa expression and occurrence of a new colorectal event was performed by Kaplan-Meier curves and log rank test.
- the time to event was defined as the time interval between the diagnosis of hyperplastic polyp and the occurrence of metachronous colorectal adenoma in the same site as the first hyperplastic polyp.
- the log- rank test was also used to assess significance of clinical characteristics. Quantitative variables were recorded into two-class variables using the median. To demonstrate that FAPa was a prognostic factor independent from other clinical factors, we performed a cox proportional- hazards model to test the simultaneous influence on disease free survival of all covariate with a p-value ⁇ 0,20 in the univariate analysis. After a backward-stepwise selection, only significant variables (p ⁇ 0.05) were kept in the final cox model. In our study, all tests were two-sided and statistical significance was set at a P value of 0.05. Analyses were performed using STATA vl l .
- the number of FAPa-positive fibroblasts in normal colon, HP, adenomas, and adenocarcinomas are reported in figure 1.
- FAPa expression was recorded as 'no/low expression' or 'high expression' based on the number of stained fibroblasts in twenty randomly-picked microscope fields at xlOOO magnification
Abstract
The present invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step ofdetermining the level of FAPα expression in a tissue sample of a hyperplastic polyp obtained from said patient.
Description
METHOD FOR PREDICTING THE RISK OF DEVELOPING A COLONIC
NEOPLASIA
FIELD OF THE INVENTION:
The invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
BACKGROUND OF THE INVENTION:
Worldwide, colorectal cancer (CRC) is the third most frequent cancer and the fourth in terms of mortality. Its adenocarcinoma sequence is quite well established, however, confusion still remains regarding the colonic neoplasia outcome of patients presenting with a particular type of polyps, the hyperplastic polyps (HP). With a prevalence of 10% to 35%, they are the most frequent colorectal lesions in the occidental world (Huang et al, 2004). Contrary to adenomatous polyps that have long been considered as preneoplastic lesions leading to a colonoscopy follow-up for these patients, no recommendation exists for patients presenting with hyperplastic polyps at their first colonoscopy if the polyps are less than 1cm, if less than 5 of them have been resected or if there is no family history of HP (Bond, 2000). The malignant potential of hyperplastic polyps has long been unknown, but recent molecular characterization studies have provided arguments in favor of a neoplastic potential, highlighting several prooncogenic alterations in these lesions such as for example CpG Methylation, microsatellite instability (O'Brien et al, 2004; O'Brien et al, 2006). In addition, analysis of mixed polyps in the study by lino and colleagues (lino et al, 1999) showed a clonal relationship between the two epithelial components, hyperplastic and adenomatous, of these polyps. These results suggest that mixed polyps are not due to a fusion of hyperplastic and adenomatous lesions but also support the hypothesis of a continuum between HP and adenomas. Recent studies, including ours, actually report that they could represent precursor lesions of some sporadic colorectal cancers (Do et al, 2012; Goldstein et al, 2003; Huang et al, 2001).
Tumor microenvironment is now known to play a critical role in the tumoral process. Cancer-associated stroma is a complex medium where a variety of interactions between the tumor and host tissue cells take place. The tumor produces factors that will modify the stroma compartment including the stroma cells. Cancer-Associated Fibroblasts (CAFs), corresponding to fibroblasts present in the tissue stroma that are activated by signals induced by the tumor, represent the main cell population within the stroma.
FAPa (Fibroblast Activation Protein a) is a type II transmembrane serine protease glycoprotein expressed in more than 90% of human epithelial cancers. In epithelial-derived tumors, it is expressed by CAFs and not by the cancer epithelial cells themselves, and represents a marker of the activation of the surrounding fibroblasts by the tumor (Montironi et al, 1996; Park et al, 1999). A previous study conducted on stage I to stage IV colon cancer patients, described an inversed correlation between FAPa expression and tumor stage but also with tumor size suggesting an implication of the glycoprotein in early steps of the disease (Henry et al, 2007). Thus FAPa could represent an early bio marker for CRC.
SUMMARY OF THE INVENTION:
The inventors conducted a 10-year retrospective study on a characterized HP patient cohort (Do et al, 2012) to examine FAPa expression in HP. They show that FAPa expression in colon fibroblasts represents a bio marker allowing predicting the risk of colonic neoplasia in patients presenting with hyperplastic colonic polyps. More precisely, the inventors show in patients, without history of colorectal pathology, presenting initial HP which are considered as non neoplastic (size < 1 cm and number < 5), that FAPa expression is significantly higher in HP compared to normal colonic mucosa.
Thus, the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
DETAILED DESCRIPTION OF THE INVENTION:
Risk method
The invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
More particularly, the invention relates to an in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient. Particularly, the invention relates to an in vitro method for determining which patient having hyperplastic polyps will develop a colonic neoplasia (adenomas, adenocarcinomas) after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of an hyperplastic polyp obtained from said patient.
As used herein, "FAPa" for "Fibroblast Activation Protein a" denotes a type II transmembrane serine protease glycoprotein expressed in more than 90% of human epithelial cancers. The amino acid sequence of FAPa is described in NCBI database under accession number NP 004451.2 and is also described as the amino acid sequence SEQ ID NO 1.
SEP ID NO 1 : MKTWVKIVFG VATSAVLALL VMCIVLRPSR VHNSEENTMR ALTLKDILNG TFSYKTFFPN WISGQEYLHQ SADNNIVLYN IETGQSYTIL SNRTMKSVNA SNYGLSPDRQ FVYLESDYSK LWRYSYTATY YIYDLSNGEF VRGNELPRPI QYLCWSPVGS KLAYVYQNNI YLKQRPGDPP FQITFNGREN KIFNGIPDWV YEEEMLATKY ALWWSPNGKF LAYAEFNDTD IPVIAYSYYG DEQYPRTINI PYPKAGAKNP VVRIFIIDTT YPAYVGPQEV PVPAMIASSD YYFSWLTWVT DERVCLQWLK RVQNVSVLSI CDFREDWQTW DCPKTQEHIE ESRTGWAGGF FVSTPVFSYD AISYYKIFSD KDGYKHIHYI KDTVENAIQI TSGKWEAINI FRVTQDSLFY SSNEFEEYPG RRNIYRISIG SYPPSKKCVT CHLRKERCQY YTASFSDYAK YYALVCYGPG IPISTLHDGR TDQEIKILEE NKELENALKN IQLPKEEIKK LEVDEITLWY KMILPPQFDR SKKYPLLIQV YGGPCSQSVR SVFAVNWISY LASKEGMVIA LVDGRGTAFQ GDKLLYAVYR KLGVYEVEDQ ITAVRKFIEM GFIDEKRIAI WGWSYGGYVS SLALASGTGL FKCGIAVAPV SSWEYYASVY TERFMGLPTK DDNLEHYKNS TVMARAEYFR
NVDYLLIHGT ADDNVHFQNS AQIAKALVNA QVDFQAMWYS DQNHGLSGLS TNHLYTHMTH FLKQCFSLSD.
As used herein, the term "colonic neoplasia" or "colonic neoplasm" denotes a tissue whose cells have lost its normal differentiation with abnormalities of nucleus and/or proliferation present in the large intestine (colon, cecum, rectum) including colorectal adenomas (including tubular, villous, tubulovillous and serrated adenomas) and adenocarcinomas.
As used herein, the term "hyperplastic polyp" denotes a non neoplastic polyp of the large intestine (colon, cecum, rectum) including globlet cell-rich HP, microvesicular HP and mucin poor HP with or without abnormal proliferation [WHO Classification of Tumours of the Digestive System, Fourth Edition and WHO Classification of Tumours, Volume 3 IARC Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D].
According to the invention, the tissue sample of a hyperplastic polyp may be obtained in the distal or proximal colon, as well as in the cecum or rectum.
In one embodiment, the tissue sample is fibroblasts. In a particular embodiment, the fibroblasts are cancer-associated fibroblast (CAFs). The tissue samples may be obtained from hyperplastic polyps preserved by methods classically used by anatomopathology department, e.g. paraffin embedded or frozen tissues.
In a particular embodiment, the method is applied on a patient with hyperplastic polyps for which no endoscopic surveillance is recommended neither in the guidelines from the French National Agency for Accreditation and Evaluation in Healthcare, nor by the American College of Gastroenterology (polyp size lower than 1 cm, less than 5 hyperplastic polyps and no family history of hyperplastic polyps).
The term "determining the level of FAPa expression" as used above includes qualitative and/or quantitative detection (measuring levels) with or without reference to a control. Typically, FAPa expression may be measured for example by RT-PCR or immunohistochemistry performed on the sample.
Preferably, the invention relates to a method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia in a patient comprising a step a) consisting of measuring FAPa expression in a sample obtained from said patient. Preferably, the method of the invention further comprises a step of comparing FAPa expression level obtained in step a) to a threshold level.
The "control" may be a healthy subject, i.e. a subject who does not suffer from any colonic neoplasia. The control may also be a subject suffering from colonic neoplasia. Preferably, said control is a healthy subject.
For example, detecting FAPa expression in sample may be performed by measuring the expression level of FAPa gene.
Typically, the detection comprises contacting the sample with selective reagents such as probes, primers or ligands, and thereby detecting the presence, or measuring the amount, of polypeptides or nucleic acids of interest originally present in the sample. Contacting may be performed in any suitable device, such as a plate, microtiter dish, test tube, well, glass, column. In specific embodiments, the contacting is performed on a substrate coated with the reagent, such as a nucleic acid array or a specific ligand array. The substrate may be a solid or semi-solid substrate such as any suitable support comprising glass, plastic, nylon, paper, metal, polymers and the like. The substrate may be of various forms and sizes, such as a slide, a membrane, a bead, a column, a gel, etc. The contacting may be made under any condition suitable for a detectable complex, such as a nucleic acid hybrid or an antibody-antigen complex, to be formed between the reagent and the nucleic acids or polypeptides of the sample.
In a particular embodiment, the expression level of FAPa gene may be determined by determining the quantity of mRNA of FAPa gene. Such method may be suitable to measure the expression level of FAPa gene in the sample.
Methods for measuring the quantity of mRNA are well known in the art. For example the nucleic acid contained in the samples (e.g., cell or tissue prepared from the patient) is first extracted according to standard methods, for example using lytic enzymes or chemical solutions or extracted by nucleic-acid-binding resins following the manufacturer's instructions. The extracted mRNA may be then detected by hybridization (e. g., Northern blot analysis).
Alternatively, the extracted mRNA may be subjected to coupled reverse transcription and amplification, such as reverse transcription and amplification by polymerase chain reaction (RT-PCR), using specific oligonucleotide primers that enable amplification of a
region in FAPa gene. Preferably quantitative or semi-quantitative RT-PCR is used. Real-time quantitative or semi-quantitative RT-PCR is particularly advantageous. Extracted mRNA may be reverse-transcribed and amplified, after which amplified sequences may be detected by hybridization with a suitable probe or by direct sequencing, or any other appropriate method known in the art.
Other methods of amplification include ligase chain reaction (LCR), transcription- mediated amplification (TMA), strand displacement amplification (SDA) and nucleic acid sequence based amplification (NASBA).
Nucleic acids having at least 10 nucleotides and exhibiting sequence complementarity or homology to the mRNA of interest herein find utility as hybridization probes or amplification primers. It is understood that such nucleic acids need not be identical, but are typically at least about 80% identical to the homologous region of comparable size, more preferably at least 85% identical and even more preferably at least 90%, preferably at least 95% identical. In certain embodiments, it will be advantageous to use nucleic acids in combination with appropriate means, such as a detectable label, for detecting hybridization. A wide variety of appropriate indicators are known in the art including, fluorescent, radioactive, enzymatic or other ligands (e. g. avidin/biotin).
Probes typically comprise single-stranded nucleic acids of between 10 to 1000 nucleotides in length, for instance of between 10 and 800, more preferably of between 15 and 700, typically of between 20 and 500. Primers typically are shorter single- stranded nucleic acids, of between 10 to 25 nucleotides in length, designed to perfectly or almost perfectly match a nucleic acid of interest, to be amplified. The probes and primers are "specific" to the nucleic acids they hybridize to, i.e. they preferably hybridize under high stringency hybridization conditions (corresponding to the highest melting temperature Tm, e.g., 50 % formamide, 5x or 6x SCC. SCC is a 0.15 M NaCl, 0.015 M Na-citrate).
In a particular embodiment, the method of the invention comprises the steps of providing total RNAs obtained from the sample of the patient, and subjecting the RNAs to amplification and hybridization to specific probes, more particularly by means of a quantitative or semi-quantitative RT-PCR.
Total RNAs can be easily extracted from the sample. For instance, the sample may be treated prior to its use, e.g. in order to render nucleic acids available. Techniques of cell or protein lysis, concentration or dilution of nucleic acids, are known by the skilled person.
In another embodiment, the expression level of FAPa gene may be measured by DNA microarray analysis. Such DNA microarray or nucleic acid microarray consists of different
nucleic acid probes that are chemically attached to a substrate, which can be a microchip, a glass slide or a microsphere-sized bead. A microchip may be constituted of polymers, plastics, resins, polysaccharides, silica or silica-based materials, carbon, metals, inorganic glasses, or nitrocellulose. Probes comprise nucleic acids such as cDNAs or oligonucleotides that may be about 10 to about 60 base pairs. To measure the expression level of FAPa gene, a sample from a test subject, optionally first subjected to a reverse transcription, is labelled and contacted with the microarray in hybridization conditions, leading to the formation of complexes between target nucleic acids that are complementary to probe sequences attached to the microarray surface. The labelled hybridized complexes are then detected and can be quantified or semi-quantified. Labelling may be achieved by various methods, e.g. by using radioactive or fluorescent labelling. Many variants of the microarray hybridization technology are available to the man skilled in the art (see e.g. the review by Hoheisel, Nature Reviews, Genetics, 2006, 7:200-210). Determine the FAPa expression in the tissue sample of a hyperplastic polyp may be performed by determining the expression level of FAPa protein. Any methods that permit to determine the expression of a specific protein in tissues can be used.
Such methods comprise contacting a tissue sample of a hyperplastic polyp sample with a binding partner capable of selectively interacting with FAPa present in the sample. The binding partner may be an antibody polyclonal or monoclonal, an antibody fragment, synthetic antibodies, or other protein- specific agents such as nucleic acid or peptide aptamers. Preferably, the binding partner is a polyclonal or monoclonal antibody.
A particular method according to the present invention is immunohistochemistry analysis. Antibodies specific for FAPa are preferred for this purpose due to specificity and availability. Several laboratories have generated and characterized specific FAPa antibodies. In addition, such antibodies may be easily generated using techniques well-known to those skilled in the art. The use of antibodies to identify proteins of interest in the cells of a tissue, referred to as immunohistochemistry (IHC), is well established. See for exemple "Principles and practice of immunoassays" 1991, CP. Price and D.J. Neoman (eds) Stockton Press, N.Y.
For the detection of the antibody that makes the presence of the protein of interest detectable by microscopy or an automated analysis system, FAPa antibodies may be tagged directly with detectable labels such as enzymes, chromogens or fluorescent probes or indirectly detected with a secondary antibody conjugated with detectable labels. A particular
staining method according to the present invention uses a secondary antibody coupled to an amplification system (to intensify staining signal) and enzymatic molecules. Such coupled secondary antibodies are commercially available, e.g. from Dako, EnVision system. Counterstaining may be used, e.g. H&E, DAPI, Hoechst.
Other staining methods may be accomplished using any suitable method or system as would be apparent to one of skill in the art, including automated, semi-automated or manual systems. The method further comprise a step consisting of comparing the expression level of
FAPa in the sample with a reference value or threshold value, wherein a difference between said expression level and said reference value is indicative of risk of developing a colonic neoplasia.
In other word, the method further comprise a step consisting of comparing the expression level of FAPa in the sample with a reference value, wherein a difference between said expression level and said reference value is predictive of development of a colonic neoplasia after resection of the HP.
Typically, a "threshold value" or "cut-off value" can be determined experimentally, empirically, or theoretically. A threshold value can also be arbitrarily selected based upon the existing experimental and/or clinical conditions, as would be recognized by a person of ordinary skilled in the art. The threshold value has to be determined in order to obtained the optimal sensitivity and specificity according to the function of the test (screening, diagnostic, predictive or prognostic) and the benefice/risk balance (clinical consequences of false positive and false negative). Typically, the optimal sentivity and specificity (and so the threshold value) can be determined using a Receiver Operating Characteristic (ROC) curve based on experimental data. Preferably, the person skilled in the art may compare the expression levels of FAPa obtained according to the method of the invention with a defined threshold value. In a particular embodiment, the method comprises quantification of the expression of
FAPa. The expression of the FAPa protein is determined by the percentage of fibroblasts cells in the whole hyperplastic polyp that express the FAPa protein.
In other word, to apply the method according to the invention, the number of positives fibroblasts for FAPa is determined.
In a particular embodiment, the fibroblasts are cancer-associated fibroblast (CAFs).
The inventors have established that patients could be at no/low or high risk of colonic neoplastic events when the number of stained fibroblasts was respectively inferior or equal/superior at 9. They also considered 9 stained fibroblasts as a threshold for no/low or a high expression of the protease in HP.
The inventors also show that patients with no/low expression of FAPa (number of stained fibroblasts inferior at 9) have 91% of neoplasm free-survival at 5 years whereas patients with high expression of FAPa (number of stained fibroblasts equal/superior at 9) have 41% of neoplasm free-survival at 5 years (see figure 3).
In these studies, the measure of FAPa has been performed by immunohistochemistry.
The inventors have established that the association between FAPa staining and neoplasm-free survival is independent from the subject's age, HP localisation and HP size, by performing multivariate analysis (table 2). After adjustment, FAPa expression was still highly significantly associated with adenoma occurrences (p<0.022). Taken together, these results show that FAPa staining in HP is a strong independent prognostic factor.
The present invention also relates to kits for performing the method according to the invention comprising means for determining the level of FAPa expression.
According to the invention, the kits of the invention may comprise an anti- FAPa antibody; and another molecule coupled with a signalling system which binds to said FAPa antibody.
Typically, the antibodies or combination of antibodies are in the form of solutions ready for use. In one embodiment, the kit comprises containers with the solutions ready for use. Any other forms are encompassed by the present invention and the man skilled in the art can routinely adapt the form to the use in immunohistochemistry. The present invention also relates to FAPa as a bio marker for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia.
In other word, the present invention relates to FAPa as a biomarker for determining whether a patient having hyperplastic polyps will develop a colonic neoplasia (adenomas, adenocarcinomas) after resection of said polyp.
Predicting method
In another aspect, the invention relates to a method for predicting the survival time of a patient having hyperplastic polyps comprising the steps consisting of i) determining the level expression of FAPa in a tissue sample from said patient, ii) comparing said level expression with a predetermined reference value and iii) providing a good prognosis of the survival time when the level expression is lower than the predetermined reference value and a poor prognosis of the survival time when the level expression is higher than the predetermined reference value.
In one embodiment, the tissue sample is fibroblasts. In a particular embodiment, the fibroblasts are cancer-associated fibroblast (CAFs).
In another embodiment, the number of positives fibroblasts for FAPa is determined.
The tissue samples may be obtained from hyperplastic polyps preserved by methods classically used by anatomopathology department, e.g. paraffin embedded or frozen tissues.
Determining the level expression of the marker of the invention may be determined by any well known method in the art and described above. Typically, such methods comprise contacting the tumor tissue sample with at least one selective binding agent capable of selectively interacting with the markers of the invention. The selective binding agent may be polyclonal antibody or monoclonal antibody, an antibody fragment, synthetic antibodies, or other protein- specific agents such as nucleic acid or peptide aptamers. Typically, the selective binding agent binds any of the markers, such as an antibody specific for any of these molecules. Several antibodies have been described in the prior art and many antibodies are also commercially available such as described in the EXAMPLE. For the detection of the antibody that makes the presence of the markers detectable by microscopy or an automated analysis system, the antibodies may be tagged directly with detectable labels such as enzymes, chromogens or fluorescent probes or indirectly detected with a secondary antibody conjugated with detectable labels.
A particular method according to the present invention is immunohistochemistry as explained above.
Therapeutic method
In another aspect, the invention relates to a method of prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention by administrating an antagonist of FAPa.
In another embodiment, the invention relates to a method of prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention by administrating an antagonist of FAPa.
In another embodiment, the invention relates to an antagonist of FAPa for use in a prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention.
In another embodiment, the invention relates to an antagonist of FAPa for use in a prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
As used herein, the term "method of prophylactic treatment" denotes a treatment which permits to a patient to not have a colonic neoplasia after resection. In other word, the "prophylactic treatment" is a preventive treatment.
As used herein, the term "antagonist of FAPa" denotes a small organic molecule, an antibody anti-FAPa, an aptamer anti-FAPa, or an inhibitor of the FAPa activity [see for review Kelly et al, 2012, Ellen Pure 2009 or Rui Liu et al, 2012 which are incorporated by reference into the present disclosure].
As used herein, the term "inhibitor of the FAPa activity" denotes molecule which is capable of inhibiting the enzymatic activity of FAPa for example, a molecule which is capable of inhibiting the cleavage of c AP or the SPRY2 protein, two substrates of FAPa [for review about FAPa see Kelly et al, 2012].
In one embodiment, said antagonist of FAPa may be a low molecular weight antagonist, e. g. a small organic molecule (natural or not).
The term "small organic molecule" refers to a molecule (natural or not) of a size comparable to those organic molecules generally used in pharmaceuticals. The term excludes biological macromolecules (e. g., proteins, nucleic acids, etc.). Preferred small organic molecules range in size up to about 10000 Da, more preferably up to 5000 Da, more preferably up to 2000 Da and most preferably up to about 1000 Da.
In one embodiment, the antagonist may bind to FAPa and block the binding of other compound on FAPa or the activity of FAPa. For example, the peptidyl chloromethyl ketones or the Phe-Arg-(8-amino-3,6-dioxaoctanoic acid)-Gly-[r]-fluoropyrrolidide may be used as inhibitors of FAPa activity [for examples see Kelly et al, 2012]. Others molecules like boronic acid-based inhibitors such as Val-boroPro, Pro-boroPro, Glu-boroPro and Ala-boroPro may be useful as antagonist [see Kelly et al, 2012 or Rui Liu et al., 2012].
In another embodiment, antagonist of FAPa of the invention may be an anti- FAPa antibody which neutralizes FAPa or an anti- FAPa fragment thereof which neutralizes FAPa.
Antibodies directed against FAPa can be raised according to known methods by administering the appropriate antigen or epitope to a host animal selected, e.g., from pigs, cows, horses, rabbits, goats, sheep, and mice, among others. Various adjuvants known in the art can be used to enhance antibody production. Although antibodies useful in practicing the invention can be polyclonal, monoclonal antibodies are preferred. Monoclonal antibodies against FAPa can be prepared and isolated using any technique that provides for the production of antibody molecules by continuous cell lines in culture. Techniques for production and isolation include but are not limited to the hybridoma technique originally described by Kohler and Milstein (1975); the human B-cell hybridoma technique (Cote et al, 1983); and the EBV-hybridoma technique (Cole et al. 1985). Alternatively, techniques described for the production of single chain antibodies (see e.g., U.S. Pat. No. 4,946,778) can be adapted to produce anti-FAPa single chain antibodies. FAPa antagonists useful in practicing the present invention also include anti-FAPa antibody fragments including but not limited to F(ab')2 fragments, which can be generated by pepsin digestion of an intact antibody molecule, and Fab fragments, which can be generated by reducing the disulfide bridges of the F(ab')2 fragments. Alternatively, Fab and/or scFv expression libraries can be constructed to allow rapid identification of fragments having the desired specificity to FAPa.
Humanized anti-FAPa antibodies and antibody fragments therefrom can also be prepared according to known techniques. "Humanized antibodies" are forms of non-human (e.g., rodent) chimeric antibodies that contain minimal sequence derived from non-human
immunoglobulin. For the most part, humanized antibodies are human immunoglobulins (recipient antibody) in which residues from a hypervariable region (CDRs) of the recipient are replaced by residues from a hypervariable region of a non-human species (donor antibody) such as mouse, rat, rabbit or nonhuman primate having the desired specificity, affinity and capacity. In some instances, framework region (FR) residues of the human immunoglobulin are replaced by corresponding non-human residues. Furthermore, humanized antibodies may comprise residues that are not found in the recipient antibody or in the donor antibody. These modifications are made to further refine antibody performance. In general, the humanized antibody will comprise substantially all of at least one, and typically two, variable domains, in which all or substantially all of the hypervariable loops correspond to those of a non-human immunoglobulin and all or substantially all of the FRs are those of a human immunoglobulin sequence. The humanized antibody optionally also will comprise at least a portion of an immunoglobulin constant region (Fc), typically that of a human immunoglobulin. Methods for making humanized antibodies are described, for example, by Winter (U.S. Pat. No. 5,225,539) and Boss (Celltech, U.S. Pat. No. 4,816,397).
Then, for this invention, neutralizing antibodies of FAPa are selected.
In a particular embodiment, the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application WO02083171.
In a particular embodiment, the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application US2002099180.
In a particular embodiment, the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application WOO 168708.
In a particular embodiment, the antibody anti-FAPa according to the invention may be an antibody as explained in the patent application DEI 0013286.
In a particular embodiment, the antibody anti-FAPa according to the invention may be the F19 antibody or his humanized version, the sibrotuzumab, as explained in Kelly et al, 2012 or Rui Liu et al., 2012.
In a particular embodiment, the antibody anti-FAPa according to the invention may be the FAP5-DM1 antibody as explained in Rui Liu et al, 2012.
In still another embodiment, FAPa antagonists may be selected from aptamers. Aptamers are a class of molecule that represents an alternative to antibodies in term of molecular recognition. Aptamers are oligonucleotide or oligopeptide sequences with the capacity to recognize virtually any class of target molecules with high affinity and specificity. Such ligands may be isolated through Systematic Evolution of Ligands by Exponential enrichment (SELEX) of a random sequence library, as described in Tuerk C. and Gold L., 1990. The random sequence library is obtainable by combinatorial chemical synthesis of DNA. In this library, each member is a linear oligomer, eventually chemically modified, of a unique sequence. Possible modifications, uses and advantages of this class of molecules have been reviewed in Jayasena S.D., 1999. Peptide aptamers consists of a conformationally constrained antibody variable region displayed by a platform protein, such as E. coli Thioredoxin A that are selected from combinatorial libraries by two hybrid methods (Colas et al, 1996).
Then, for this invention, neutralizing aptamers of FAPa are selected.
In another embodiment, a peptide like the Melittin or the promelittin may be used to selectively killed FAPa expressing cells [see Kelly et al, 2012].
Another object of the invention relates to an antagonist of FAPa for use in the prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
In another embodiment, the invention relates to an antagonist of FAPa for use in the prophylactic treatment of patient which will develop a colonic neoplasia after resection identified with the method according to the invention.
Compounds of the invention may be administered in the form of a pharmaceutical composition, as defined below.
Preferably, said compound is an antagonist of FAPa.
By a "therapeutically effective amount" is meant a sufficient amount of compound to treat and/or to prevent a colonic neoplasia after resection.
It will be understood that the total daily usage of the compounds and compositions of the present invention will be decided by the attending physician within the scope of sound medical judgment. The specific therapeutically effective dose level for any particular patient will depend upon a variety of factors including the disorder being treated and the severity of the disorder; activity of the specific compound employed; the specific composition employed, the age, body weight, general health, sex and diet of the patient; the time of administration, route of administration, and rate of excretion of the specific compound employed; the duration of the treatment; drugs used in combination or coincidental with the specific antagonist employed; and like factors well known in the medical arts. For example, it is well within the skill of the art to start doses of the compound at levels lower than those required to achieve the desired therapeutic effect and to gradually increase the dosage until the desired effect is achieved. However, the daily dosage of the products may be varied over a wide range from 0.01 to 1,000 mg per adult per day. Preferably, the compositions contain 0.01, 0.05, 0.1, 0.5, 1.0, 2.5, 5.0, 10.0, 15.0, 25.0, 50.0, 100, 250 and 500 mg of the active ingredient for the symptomatic adjustment of the dosage to the patient to be treated. A medicament typically contains from about 0.01 mg to about 500 mg of the active ingredient, preferably from 1 mg to about 100 mg of the active ingredient. An effective amount of the drug is ordinarily supplied at a dosage level from 0.0002 mg/kg to about 20 mg/kg of body weight per day, especially from about 0.001 mg/kg to 7 mg/kg of body weight per day.
Compounds according to the invention may be used for the preparation of a pharmaceutical composition for the prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to the invention.
Hence, the present invention also provides a pharmaceutical composition comprising an effective dose of an antagonist of FAPa according to the invention.
Any therapeutic agent of the invention may be combined with pharmaceutically acceptable excipients, and optionally sustained-release matrices, such as biodegradable polymers, to form therapeutic compositions.
"Pharmaceutically" or "pharmaceutically acceptable" refers to molecular entities and compositions that do not produce an adverse, allergic or other untoward reaction when administered to a mammal, especially a human, as appropriate. A pharmaceutically acceptable carrier or excipient refers to a non-toxic solid, semi-solid or liquid filler, diluent, encapsulating material or formulation auxiliary of any type.
The form of the pharmaceutical compositions, the route of administration, the dosage and the regimen naturally depend upon the condition to be treated, the severity of the illness, the age, weight, and sex of the patient, etc.
The pharmaceutical compositions of the invention can be formulated for a topical, oral, intranasal, parenteral, intraocular, intravenous, intramuscular or subcutaneous administration and the like.
Preferably, the pharmaceutical compositions contain vehicles which are pharmaceutically acceptable for a formulation capable of being injected. These may be in particular isotonic, sterile, saline solutions (monosodium or disodium phosphate, sodium, potassium, calcium or magnesium chloride and the like or mixtures of such salts), or dry, especially freeze-dried compositions which upon addition, depending on the case, of sterilized water or physiological saline, permit the constitution of injectable solutions.
The doses used for the administration can be adapted as a function of various parameters, and in particular as a function of the mode of administration used, of the relevant pathology, or alternatively of the desired duration of treatment.
In addition, other pharmaceutically acceptable forms include, e.g. tablets or other solids for oral administration; time release capsules; and any other form currently can be used.
The invention will be further illustrated by the following figures and examples. However, these examples and figures should not be interpreted in any way as limiting the scope of the present invention. FIGURES:
Figure 1: FAPa-expression in normal, HP, low-grade dysplasia tubular adenoma (TA), high-grade dysplasia TA, and adenocarcinoma
Number of FAPa-positive fibroblats in normal colon, hyperplastic polyps (HP), low- grade dysplasia tubular adenoma (TA), high-grade dysplasia TA, and adenocarcinoma (ADC). A Wilcoxon Cuzick trend test was performed to compare the number of FAPa- positive fibroblasts between the different types of colon tissues.
Figure 2: A predictive test for recurrence - Receiver Operating Characteristic (ROC) curves for FAPa staining
'a' threshold, corresponding to the number of 9 or more FAPD -stained fibroblasts in HP, had a sensitivity of 81.25% and a specificity of 87.93% that actually represents the optimal sensitivity and specificity couple. Se, sensitivity; Spe, specificity.
Figure 3: Kaplan-Meier survival estimate based on the number of FAPa expression in HP patients
Neoplasm-free survival among patients with colonoscopy follow-up according to FAPa expression. P-value corresponds to logrank univariate analysis.
Table 1. Clinical and immunohistological features

NOTE: FAPa expression was recorded as "No/low expression" or "high expression" based on the number of stained fibroblasts counted in 20 randomly picked microscope fields at XI 000 magnification. The threshold of FAPa expression in HP was determined to be 9
stained fibroblasts, 9 corresponding to the optimal specificity/sensibility couple based on the ROC analysis,
95% CI: Bionomial exact 95% confidence index was calculated for each percentage. Table 2. Neoplasm-free survival according to clinical and immunohistological features
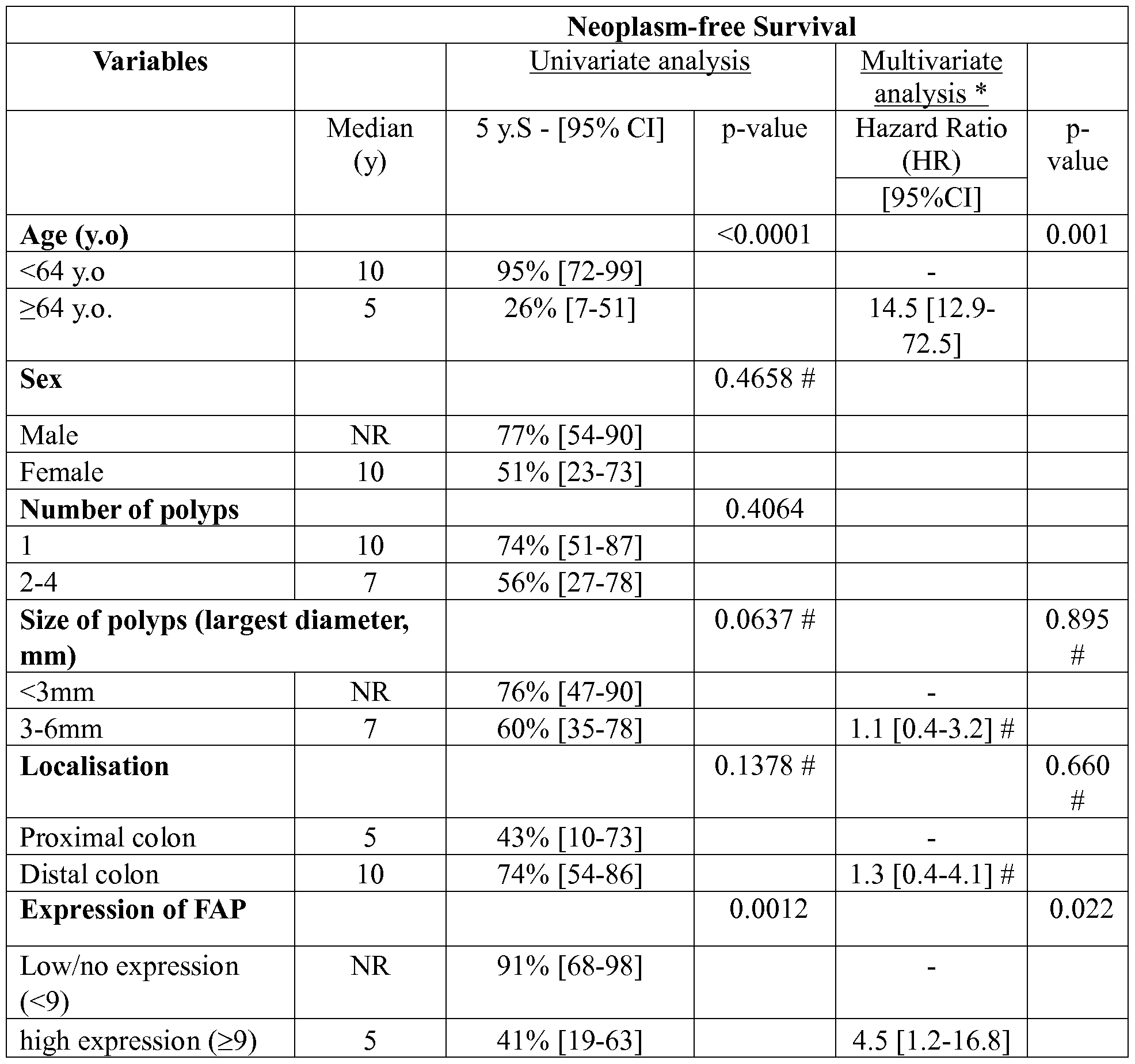
Note: Neoplam-Free Survival among patients with colonic hyperplastic polyps who had a colonoscopic follow-up. Multivariate analysis was conducted using a Cox model including all variables with a P value <0.20 in the univariate analysis.
* The initial Cox model included the age, the size, the localisation of the polyps and FAPa expression. Final model was obtained after backward stepwise selection, keeping only
the variables with a P value <0.05 (i.e. age and FAPa). 95% CI was calculated for all 5-year survival values.
# HR and p-values from the initial model was provided for information for nonsignificant covariates.
EXAMPLE: Material & Methods
Study design
We conducted a single centre historical cohort study.
Sample size, patients and data collection
The FAPa staining has been done on colon tissue sections from 64 patients. 39 patients had colon hyperplastic polyps, 6 had low grade adenomas, 4 presented with high grade adenomas and 5 displayed adenocarcinomas. FAP staining was also examined on normal tissue sections from 10 patients with resected non complicated diverticula. The characteristic of the 39 patients presenting with HP have been previously published (Do et al, 2012). These 39 patients were diagnosed for HP in the Pathology department of Rangueil Hospital in 2000 and 2001. None of these patients had preceding colorectal adenocarcinoma or adenoma, familial colorectal adenocarcinoma history, hyperplastic polyposis, chronic inflammatory bowel disease, insufficient colon site information or follow-up data. In addition, none of the patients included in the study showed evidence of colonic adenoma at the initial colonoscopy. Finally, colonoscopy follow-up data were available allowing us to investigate the correlation between the neoplasm-free survival and FAPa staining in HP. Follow up colonoscopies have been done for surveillance purpose without particular colorectal pathology as mentioned in the exclusion criteria above. Approval of an institutional research ethics committee was obtained in accordance with the precepts of the Helsinki Declaration.
Immunohistochemistry
The resected tissues were formaldehyde- fixed and paraffin embedded. Citrate buffer was used for epitope retrieval. The antibodies were applied overnight and detection was done using the DakoCytomation Envision Plus System-HRP. The anti-FAPa antibody (Abeam,
ab53066) was used for all the study at a 1 :200 dilution. FAPa staining was measured by the number of stained fibroblasts in twenty fields at xlOOO magnification. Each field was chosen randomly. The staining analyses have been performed in a double blinded fashion under the supervision of pathologists. Because the inter-rater agreement was excellent (ICC=0.93), percentages were reported as the average between the two readers.
Statistical analysis
FAPa expression was recorded as 'no/low expression' or 'high expression' based on the number of stained fibroblasts counted in twenty randomly chosen microscope fields of the polyp section at XlOOO magnification. For patients with several polyps, the polyp with the wider hyperplastic area was retained for evaluation. Based on the receiver operating characteristic analysis, we found that the optimal specificity/sensibility couple corresponds to a threshold of 9 FAPa-stained fibroblasts. Thus, we established that the overexpression threshold corresponds to a number of stained fibroblasts in hyperplastic polyp equal or higher than 9. The association between FAPa expression and occurrence of a new colorectal event was performed by Kaplan-Meier curves and log rank test. The time to event was defined as the time interval between the diagnosis of hyperplastic polyp and the occurrence of metachronous colorectal adenoma in the same site as the first hyperplastic polyp. The log- rank test was also used to assess significance of clinical characteristics. Quantitative variables were recorded into two-class variables using the median. To demonstrate that FAPa was a prognostic factor independent from other clinical factors, we performed a cox proportional- hazards model to test the simultaneous influence on disease free survival of all covariate with a p-value<0,20 in the univariate analysis. After a backward-stepwise selection, only significant variables (p<0.05) were kept in the final cox model. In our study, all tests were two-sided and statistical significance was set at a P value of 0.05. Analyses were performed using STATA vl l .
Results
FAPa expression in normal colon, hyperplastic polyps, adenomas and adenocarcinomas
The number of FAPa-positive fibroblasts in normal colon, HP, adenomas, and adenocarcinomas are reported in figure 1. In the whole cohort, the number of FAPa
expressing fibroblast is 10.33±1.394 (n=64). The average number of FAPa-positive fibroblasts in normal colon from noncomplicated diverticula (2.750± 0.588, n=10) was significantly different from the number in HP (7.885±1.056, n=39, p=0.0195), low grade adenoma (11.92±1.044, n=6, p<0.0001), high grade adenoma (24.50±9.515, n=4, p=0.0025) and adenocarcinoma (31.30±7.782, n=5, p<0.0001). A significant difference was also found between HP and high grade adenoma (p=0.0004) or adenocarcinoma (p<0.0001) while none was observed between HP and low grade adenoma.
Correlation study of FA Pa expression and neoplasm-free survival in patient with hyperplastic polyps
In order to determine whether or not FAPa expression by fibroblasts could represent a bio marker predicting the risk of colonic neoplasia in patients presenting with hyperplastic polyps, we then focused our study on these colonic lesions.
To assess whether a predictive test using FAPa as a biomarker can predict the neoplasm occurrence after developing a first hyperplastic polyp, we performed a receiver operating characteristic analysis for the number of FAPa-positive fibroblast. The evaluation of the area under the curve (AUC) gave a predictive performance of FAPa value of 0.8658 (95% CI, 0.75-0.98). The ROC analysis showed that the optimal specificity-sensibility couple (i.e., with a 81.25 % sensitivity to detect the patients at risk to develop an adenoma and an optimal specificity corresponding to 87.93%) was obtained with a threshold of 9 stained fibroblasts (Figure 2). Thus, we hypothesized that patients could be at no/low or high risk of metachronous neoplastic events when the number of stained fibroblasts was respectively inferior or equal/superior at 9. As the average number of FAPa-positive fibroblasts was 7.885±1.056 in our sample, we also considered 9 stained fibroblasts as a threshold for no/low or a high expression of the protease in HP. Thus, FAPa expression was recorded as 'no/low expression' or 'high expression' based on the number of stained fibroblasts in twenty randomly-picked microscope fields at xlOOO magnification In this cohort of patients displaying HP, 56%> (95%>CI: 39-72) had no/low expression of the protease while in 44%> (95%>CI: 27-60) of them we observed a high FAPa expression (Table 1).
As previously reported (Do et al, 2012), survival analysis was performed using data from patients who had at least one colonoscopy during their follow up. Only occurrence of metachronous adenoma at the same general area of the colon (proximal or distal colon) was considered as a recurrence event. Based on this criteria, 41%> (95%>CI: 26-59) of the patients presenting with HP developed metachronous adenoma (Table 1). Univariate analysis (Table
2) showed a significant association between FAPa overexpression and shortened neoplasm- free survival (p= 0.0012). The 5 year neoplasm-free survival for patients with no/low expression of the protease was 91% (95%CI: 68-98) while it only reaches 41% (95%CI: 19- 63) for patients with high expression (Figure 3 and Table 2). Patients with high expression of FAPa had a median neoplasm- free survival of 5 years, whereas during the 10 years following period, the median survival was not reached by patients with no/low expression of FAPa (Table 2, Figure 3). To demonstrate that the association between FAPa staining and neoplasm- free survival was independent from the subject's age, we performed multivariate analysis (table 2). After adjustment, FAPa expression was still significantly associated with adenoma occurrences (p=0.022).
Taken together, these results show that FAPa staining in HP is an independent prognostic factor and the threshold of 9 FAPa-stained fibroblasts represents the optimal specificity-sensitivity couple giving a predictive threshold.
REFERENCES:
Throughout this application, various references describe the state of the art to which this invention pertains. The disclosures of these references are hereby incorporated by reference into the present disclosure.
Bond JH (2000) Polyp guideline: diagnosis, treatment, and surveillance for patients with colorectal polyps. Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol 95: 3053-63.
Do C, Bertrand C, Palasse J, Delisle MB, Shulkes A, Cohen- Jonathan-Moyal E,
Ferrand A, Seva C (2012) A New Biomarker that Predicts Colonic Neoplasia Outcome in Patients with Hyperplastic Colonic Polyps. Cancer Prev Res (Phila).
Ellen Pure. The road to integrative cancer therapies: emergence of a tumor-associated fibroblast protease as a potential therapeutic target in cancer. Expert Opin. Ther. Targets (2009) 13(8):967-973.
Goldstein NS, Bhanot P, Odish E, Hunter S (2003) Hyperplastic-like colon polyps that preceded microsatellite-unstable adenocarcinomas. Am J Clin Pathol 119: 778-96.
Henry LR, Lee HO, Lee JS, Klein-Szanto A, Watts P, Ross EA, Chen WT, Cheng JD (2007) Clinical implications of fibroblast activation protein in patients with colon cancer. Clin Cancer Res 13: 1736-41.
Huang CS, O'Brien M J, Yang S, Farraye FA (2004) Hyperplastic polyps, serrated adenomas, and the serrated polyp neoplasia pathway. Am J Gastroenterol 99: 2242-55.
lino H, Jass JR, Simms LA, Young J, Leggett B, Ajioka Y, Watanabe H (1999) DNA microsatellite instability in hyperplastic polyps, serrated adenomas, and mixed polyps: a mild mutator pathway for colorectal cancer? J Clin Pathol 52: 5-9.
Kelly Thomas, Yan Huang, Avis E. Simms, and Anna Mazur. Fibroblast activation protein-a: a key modulator of the microenvironment in multiple pathologies. International Review of Cell and Molecular Biology, Volume 297 - 2012.
Montironi R, Diamanti L, Thompson D, Bartels HG, Barrels PH (1996) Analysis of the capillary architecture in the precursors of prostate cancer: recent findings and new concepts. Eur Urol 30: 191-200.
O'Brien MJ, Yang S, Clebanoff JL, Mulcahy E, Farraye FA, Amorosino M, Swan N
(2004) Hyperplastic (serrated) polyps of the colorectum: relationship of CpG island methylator phenotype and K-ras mutation to location and histologic subtype. Am J Surg Pathol 28: 423-34.
O'Brien MJ, Yang S, Mack C, Xu H, Huang CS, Mulcahy E, Amorosino M, Farraye FA (2006) Comparison of microsatellite instability, CpG island methylation phenotype, BRAF and KRAS status in serrated polyps and traditional adenomas indicates separate pathways to distinct colorectal carcinoma end points. Am J Surg Pathol 30: 1491-501.
Park JE, Lenter MC, Zimmermann RN, Garin-Chesa P, Old LJ, Rettig WJ (1999) Fibroblast activation protein, a dual specificity serine protease expressed in reactive human tumor stromal fibroblasts. J Biol Chem 274: 36505-12.
Rui Liu, Hui Li, Liang Liu, Jinpu Yu and Xiubao Ren. Fibroblast activation protein A potential therapeutic target in cancer. Cancer Biology & Therapy 13:3, 123-129; February 1 , 2012.
Claims
1. An in vitro method for determining whether a patient having hyperplastic polyps is at risk of developing a colonic neoplasia after resection of said hyperplastic polyps, said method comprising the step of determining the level of FAPa expression in a tissue sample of a hyperplastic polyp obtained from said patient.
2. The in vitro method according to claim 1 wherein the tissue sample is fibroblasts.
3. The in vitro method according to claim 2 wherein the fibroblasts are cancer-associated fibroblast (CAFs).
4. The in vitro method according to the claims 1 to 3 wherein the level of FAPa expression is determined by immunohistochemistry.
5. The in vitro method according to claims 1 to 4 wherein the colonic neoplasia is a colorectal cancer.
6. The in vitro method according to claims 1 to 4 wherein the colonic neoplasia is a colorectal adenocarcinomas or colorectal adenoma.
7. A kit for performing the method according to claim 1 which comprises means for determining the level of FAPa in a tissue sample of a hyperplastic polyp.
8. A kit according to the claim 7 wherein the mean for determining the level of FAPa expression in the sample is an antibody directed against FAPa.
9. A method of prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to claim 1 by administrating an antagonist of FAPa.
10. An antagonist of FAPa for use in a prophylactic treatment of patient with at risk of developing a colonic neoplasia after resection identified with the method according to claim 1.
11. An antagonist for use according to claim 10 wherein the antagonist is the sibrotuzumab.
12. A method for predicting the survival time of a patient having hyperplastic polyps comprising the steps consisting of i) determining the level expression of FAPa in a tissue sample from said patient, ii) comparing said level expression with a predetermined reference value and iii) providing a good prognosis of the survival time when the level expression is lower than the predetermined reference value and a poor prognosis of the survival time when the level expression is higher than the predetermined reference value.
13. The in vitro method according to claim 10 wherein the tissue sample is fibroblasts.
14. The in vitro method according to claim 11 wherein the fibroblasts are cancer- associated fibroblast (CAFs).
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP13305476 | 2013-04-12 | ||
| EP13305476.7 | 2013-04-12 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2014167083A1 true WO2014167083A1 (en) | 2014-10-16 |
Family
ID=48366294
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/EP2014/057343 WO2014167083A1 (en) | 2013-04-12 | 2014-04-11 | Method for predicting the risk of developing a colonic neoplasia |
Country Status (1)
| Country | Link |
|---|---|
| WO (1) | WO2014167083A1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11872291B2 (en) | 2016-12-14 | 2024-01-16 | Purdue Research Foundation | Fibroblast activation protein (FAP)-targeted imaging and therapy |
Citations (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816397A (en) | 1983-03-25 | 1989-03-28 | Celltech, Limited | Multichain polypeptides or proteins and processes for their production |
| US4946778A (en) | 1987-09-21 | 1990-08-07 | Genex Corporation | Single polypeptide chain binding molecules |
| US5225539A (en) | 1986-03-27 | 1993-07-06 | Medical Research Council | Recombinant altered antibodies and methods of making altered antibodies |
| WO2001068708A2 (en) | 2000-03-17 | 2001-09-20 | Boehringer Ingelheim Pharma Kg | Human and humanized fap-alpha-specific antibodies |
| DE10013286A1 (en) | 2000-03-17 | 2001-09-20 | Boehringer Ingelheim Pharma | New human humanized antibody that specifically binds to fibroblasts activating protein alpha, useful for treating cancer or tumor, and for imaging tumors associated with activated stromal fibroblasts, e.g. lung or breast cancer |
| US20020099180A1 (en) | 2000-03-17 | 2002-07-25 | Klaus Pfizenmaier | Human FAP-alpha-specific antibodies |
| WO2002083171A2 (en) | 2001-04-12 | 2002-10-24 | Boehringer Ingelheim International Gmbh | Cancer treatment by using fap-alpha specific antibodies |
| EP2071337A1 (en) * | 2007-12-10 | 2009-06-17 | F.Hoffmann-La Roche Ag | Seprase as a marker for cancer |
| US20120258119A1 (en) * | 2009-10-02 | 2012-10-11 | Christoph Renner | Anti-fibroblast activation protein antibodies and methods and uses thereof |
-
2014
- 2014-04-11 WO PCT/EP2014/057343 patent/WO2014167083A1/en active Application Filing
Patent Citations (9)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4816397A (en) | 1983-03-25 | 1989-03-28 | Celltech, Limited | Multichain polypeptides or proteins and processes for their production |
| US5225539A (en) | 1986-03-27 | 1993-07-06 | Medical Research Council | Recombinant altered antibodies and methods of making altered antibodies |
| US4946778A (en) | 1987-09-21 | 1990-08-07 | Genex Corporation | Single polypeptide chain binding molecules |
| WO2001068708A2 (en) | 2000-03-17 | 2001-09-20 | Boehringer Ingelheim Pharma Kg | Human and humanized fap-alpha-specific antibodies |
| DE10013286A1 (en) | 2000-03-17 | 2001-09-20 | Boehringer Ingelheim Pharma | New human humanized antibody that specifically binds to fibroblasts activating protein alpha, useful for treating cancer or tumor, and for imaging tumors associated with activated stromal fibroblasts, e.g. lung or breast cancer |
| US20020099180A1 (en) | 2000-03-17 | 2002-07-25 | Klaus Pfizenmaier | Human FAP-alpha-specific antibodies |
| WO2002083171A2 (en) | 2001-04-12 | 2002-10-24 | Boehringer Ingelheim International Gmbh | Cancer treatment by using fap-alpha specific antibodies |
| EP2071337A1 (en) * | 2007-12-10 | 2009-06-17 | F.Hoffmann-La Roche Ag | Seprase as a marker for cancer |
| US20120258119A1 (en) * | 2009-10-02 | 2012-10-11 | Christoph Renner | Anti-fibroblast activation protein antibodies and methods and uses thereof |
Non-Patent Citations (20)
| Title |
|---|
| "Principles and practice of immunoassays", 1991, STOCKTON PRESS |
| BOND JH: "Polyp guideline: diagnosis, treatment, and surveillance for patients with colorectal polyps. Practice Parameters Committee of the American College of Gastroenterology", AM J GASTROENTEROL, vol. 95, 2000, pages 3053 - 63 |
| BOSMAN, F.T.; CARNEIRO, F.; HRUBAN, R.H.; THEISE, N.D: "IARC", vol. 3, article "WHO Classification of Tumours of the Digestive System" |
| C. DO ET AL: "A New Biomarker That Predicts Colonic Neoplasia Outcome in Patients with Hyperplastic Colonic Polyps", CANCER PREVENTION RESEARCH, vol. 5, no. 4, 24 February 2012 (2012-02-24), pages 675 - 684, XP055033755, ISSN: 1940-6207, DOI: 10.1158/1940-6207.CAPR-11-0408 * |
| DO C; BERTRAND C; PALASSE J; DELISLE MB; SHULKES A; COHEN-JONATHAN-MOYAL E; FERRAND A; SEVA C: "A New Biomarker that Predicts Colonic Neoplasia Outcome in Patients with Hyperplastic Colonic Polyps", CANCER PREV RES (PHILA, 2012 |
| ELLEN PURE: "The road to integrative cancer therapies: emergence of a tumor-associated fibroblast protease as a potential therapeutic target in cancer", EXPERT OPIN. THER. TARGETS, vol. 13, no. 8, 2009, pages 967 - 973, XP009170364, DOI: doi:10.1517/14728220903103841 |
| GOLDSTEIN NS; BHANOT P; ODISH E; HUNTER S: "Hyperplastic-like colon polyps that preceded microsatellite-unstable adenocarcinomas", AM J CLIN PATHOL, vol. 119, 2003, pages 778 - 96 |
| HENRIKSSON MARIA L ET AL: "Colorectal Cancer Cells Activate Adjacent Fibroblasts Resulting in FGF1/FGFR3 Signaling and Increased Invasion", AMERICAN JOURNAL OF PATHOLOGY, vol. 178, no. 3, March 2011 (2011-03-01), pages 1387 - 1394, XP002698821 * |
| HENRY LR; LEE HO; LEE JS; KLEIN-SZANTO A; WATTS P; ROSS EA; CHEN WT; CHENG JD: "Clinical implications of fibroblast activation protein in patients with colon cancer", CLIN CANCER RES, vol. 13, 2007, pages 1736 - 41 |
| HERRERA MERCEDES ET AL: "Cancer-associated fibroblast and M2 macrophage markers together predict outcome in colorectal cancer patients", CANCER SCIENCE, vol. 104, no. 4, 21 February 2013 (2013-02-21), pages 437 - 444, XP002698819 * |
| HOHEISEL, NATURE REVIEWS, GENETICS, vol. 7, 2006, pages 200 - 210 |
| HUANG CS; O'BRIEN M J; YANG S; FARRAYE FA: "Hyperplastic polyps, serrated adenomas, and the serrated polyp neoplasia pathway", AM J GASTROENTEROL, vol. 99, 2004, pages 2242 - 55 |
| KELLY THOMAS; YAN HUANG; AVIS E. SIMMS; ANNA MAZUR: "Fibroblast activation protein-a: a key modulator of the microenvironment in multiple pathologies", INTERNATIONAL REVIEW OF CELL AND MOLECULAR BIOLOGY, vol. 297, 2012 |
| LINO H; JASS JR; SIMMS LA; YOUNG J; LEGGETT B; AJIOKA Y; WATANABE H: "DNA microsatellite instability in hyperplastic polyps, serrated adenomas, and mixed polyps: a mild mutator pathway for colorectal cancer?", J CLIN PATHOL, vol. 52, 1999, pages 5 - 9 |
| MONTIRONI R; DIAMANTI L; THOMPSON D; BARTELS HG; BARTELS PH: "Analysis of the capillary architecture in the precursors of prostate cancer: recent findings and new concepts", EUR UROL, vol. 30, 1996, pages 191 - 200 |
| O'BRIEN MJ; YANG S; CLEBANOFF JL; MULCAHY E; FARRAYE FA; AMOROSINO M; SWAN N: "Hyperplastic (serrated) polyps of the colorectum: relationship of CpG island methylator phenotype and K-ras mutation to location and histologic subtype", AM J SURG PATHOL, vol. 28, 2004, pages 423 - 34 |
| O'BRIEN MJ; YANG S; MACK C; XU H; HUANG CS; MULCAHY E; AMOROSINO M; FARRAYE FA: "Comparison of microsatellite instability, CpG island methylation phenotype, BRAF and KRAS status in serrated polyps and traditional adenomas indicates separate pathways to distinct colorectal carcinoma end points", AM J SURG PATHOL, vol. 30, 2006, pages 1491 - 501, XP009121216, DOI: doi:10.1097/01.pas.0000213313.36306.85 |
| PARK JE; LENTER MC; ZIMMERMANN RN; GARIN-CHESA P; OLD LJ; RETTIG WJ: "Fibroblast activation protein, a dual specificity serine protease expressed in reactive human tumor stromal fibroblasts", J BIOL CHEM, vol. 274, 1999, pages 36505 - 12, XP002163938, DOI: doi:10.1074/jbc.274.51.36505 |
| RUI LIU; HUI LI; LIANG LIU; JINPU YU; XIUBAO REN: "Fibroblast activation protein A potential therapeutic target in cancer", CANCER BIOLOGY & THERAPY, vol. 13, no. 3, 1 February 2012 (2012-02-01), pages 123 - 129 |
| WIKBERG MARIA L ET AL: "High intratumoral expression of fibroblast activation protein (FAP) in colon cancer is associated with poorer patient prognosis", TUMOR BIOLOGY, vol. 34, no. 2, 18 January 2013 (2013-01-18), pages 1013 - 1020, XP002698820 * |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US11872291B2 (en) | 2016-12-14 | 2024-01-16 | Purdue Research Foundation | Fibroblast activation protein (FAP)-targeted imaging and therapy |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US11279979B2 (en) | Method of determining PIK3CA mutational status in a sample | |
| CA2767914C (en) | Markers for endometrial cancer | |
| Min et al. | S100A4 expression is associated with lymph node metastasis in papillary microcarcinoma of the thyroid | |
| US20100190656A1 (en) | Breast Cancer Specific Markers and Methods of Use | |
| AU2010295172B2 (en) | Methods and compositions for the diagnosis and treatment of thyroid cancer | |
| AU2011250588B2 (en) | Method for the diagnosis of epithelial cancers by the detection of EpICD polypeptide | |
| AU2011250588C1 (en) | Method for the diagnosis of epithelial cancers by the detection of EpICD polypeptide | |
| CA2734519C (en) | Markers and methods for assessing and treating ulcerative colitis and related disorders using a 20 gene panel | |
| CN106662543B (en) | Non-invasive gene mutation detection in lung cancer patients | |
| AU2011250588A1 (en) | Method for the diagnosis of epithelial cancers by the detection of EpICD polypeptide | |
| CN113249491A (en) | Biomarker for diagnosing endometrial cancer and product and application thereof | |
| KR20140108718A (en) | Biomarkers for kawasaki disease | |
| JP2008535855A5 (en) | ||
| US20180355438A1 (en) | Abca1 downregulation in prostate cancer | |
| KR101475032B1 (en) | Marker for diagnosing HER2 inhibitor resistance cancer, diagnostic kit comprising the same and method for diagnosing HER2 inhibitor resistance cancer | |
| JP2009523004A5 (en) | ||
| CN112626207B (en) | Gene combination for distinguishing non-invasive and invasive non-functional pituitary adenomas | |
| EP2313526A1 (en) | Identifying cancers sensitive to treatment with inhibitors of notch signaling | |
| WO2018233511A1 (en) | Method for predicting response of esophagus cancer to anti-erbb3 antibody therapy, and kit | |
| WO2013104103A1 (en) | Colorectal cancer diagnosis and indication marker | |
| WO2014167083A1 (en) | Method for predicting the risk of developing a colonic neoplasia | |
| AU2010272370A2 (en) | Biomarker for gastrointestinal cancer | |
| EP2715364A1 (en) | Method for predicting the risk of developing a colonic neoplasia | |
| CN116411080B (en) | Marker for distinguishing cold and hot tumors | |
| US20220298565A1 (en) | Method Of Determining PIK3CA Mutational Status In A Sample |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 14716828 Country of ref document: EP Kind code of ref document: A1 |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| 122 | Ep: pct application non-entry in european phase |
Ref document number: 14716828 Country of ref document: EP Kind code of ref document: A1 |