
Abstract
Purpose
To determine whether, in obese [body mass index (BMI) > 30 kg·m2] patients, oral intake of 300 mL clear liquid two hours before elective surgery affects the volume and pH of gastric contents at induction of anesthesia.
Methods
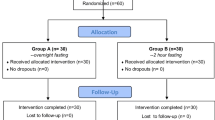
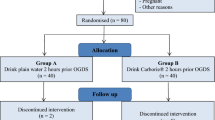
A single-blind, randomized study of 126 adult patients, age ≥18 yr, ASA physical status I or II, BMI > 30 kg·m2 who were scheduled for elective surgery under general anesthesia. Patients were excluded if they had diabetes mellitus, symptoms of gastroesophageal reflux, or had taken medication within 24 hr that affects gastric secretion, gastric fluid pH or gastric emptying. All patients fasted from midnight and were randomly assigned to fasting or fluid group. Two hours before their scheduled time of surgery, all patients drank 10 mL of water containing phenol red 50 mg. Those in the fluid group followed with 300 mL clear liquid of their choice. Immediately following induction of general anesthesia and tracheal intubation, gastric contents were aspirated through a multiorifice Salem sump tube. The fluid volume, pH and phenol red concentration were recorded.
Results
Median (range) values in fasting vs fluid groups were: gastric fluid volume 26 (3–107) mL vs 30 (3–187) mL, pH 1.78 (1.31–7.08) vs 1.77 (1.27–7.34) and phenol red retrieval 0.1 (0–30)% vs 0.2 (0–15)%. Differences between groups were not statistically significant.
Conclusion
Obese patients without comorbid conditions should follow the same fasting guidelines as non-obese patients and be allowed to drink clear liquid until two hours before elective surgery, inasmuch as obesity per se is not considered a risk factor for pulmonary aspiration.
Résumé
Objectif
Déterminer si, chez des patients obèses [indice de masse corporelle (IMC) > 30 kg·m2], la prise orale de 300 mL de liquide clair deux heures avant de subir une opération réglée a un effet sur le volume et le pH du contenu gastrique lors de l’induction anesthésique.
Méthode
Une étude randomisée, à simple insu, a été menée auprès de 126 patients adultes, ≥18 ans, d’état physique ASA I ou II, d’IMC > 30 kg·m2, devant subir une intervention chirurgicale réglée sous anesthésie générale. La présence de diabète, ou de symptômes de reflux gastro-œsophagien ou la prise de médicaments, dans les 24 h avant l’opération, pouvant affecter la sécrétion gastrique, le pH du liquide gastrique ou l’évacuation gastrique entraînaient l’exclusion du patient. Tous les patients, à jeun depuis minuit, ont été répartis en deux groupes :jeûne ou liquide. Deux heures avant l’heure prévue de l’opération, tous les patients ont bu 10 mL d’eau contenant 50 mg de rouge de phénol. Les patients du groupe «liquide» ont pris ensuite 300 mL d’un liquide clair de leur choix. Immédiatement après l’induction de l’anesthésie et l’intubation endotrachéale, le contenu gastrique a été aspiré au moyen d’une sonde multiorifice Salem. Le volume de liquide, le pH et les concentrations de rouge de phénol ont été notés.
Résultats
Les valeurs moyennes (étendue) du groupe de jeûne vs le groupe «liquide» ont été : volume de liquide gastrique 26 (3–107) mL vs 30 (3–187) mL, pH 1,78 (1,31–7,08) vs 1,77 (1,27–7,34) et repérage du rouge de phénol 0,1 (0–30) % vs 0,2 (0–15) %. Il n’y avait pas de différence intergroupe significative.
Conclusion
Les patients obèses, sans symptômes comorbides, devraient suivre les mêmes directives de jeûne que les patients non obèses. Ils peuvent boire un liquide clair jusqu’à deux heures avant une opération réglée, étant donné que l’obésité en elle-même n’est pas considérée comme un facteur de risque d’aspiration pulmonaire.
Article PDF
Similar content being viewed by others

References
Olsson GL, Hallen B, Hambraeus-Jonzon K. Aspiration during anaesthesia: a computer-aided study of 185 358 anaesthetics. Acta Anaesthesiol Scand 1986; 30: 84–92.
Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration in the perioperative period. Anesthesiology 1993; 78: 59–62.
Fasting S, Gisvold SE. Serious intraoperative problems-a five-year review of 83,844 anesthetics. Can J Anesth 2002; 49: 545–53.
Anonymous. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: a report by the American Society of Anesthesiologist Task Force on Preoperative Fasting. Anesthesiology 1999; 90: 896–905.
Vaughan RW, Bauer S, Wise L. Volume and pH of gastric juice in obese patients. Anesthesiology 1975; 43: 686–9.
Harter RL, Kelly WB, Kramer MG, Perez CE, Dzwonczyk RR. A comparison of the volume and pH of gastric contents of obese and lean surgical patients. Anesth Analg 1998; 86: 147–52.
Katzmarzyk PT. The Canadian obesity epidemic: an historical perspective. Obes Res 2002; 10: 666–74.
Wadden TA, Brownell KD, Foster GD. Obesity: responding to the global epidemic. J Consult Clin Psychol 2002; 70: 510–25.
2001 CAS Guidelines to the practice of anesthesia. Can J Anesth 2001; 48(Suppl).
Horowitz M, Collins PJ, Harding PE, Shearman DJ. Abnormalities of gastric emptying in obese patients. Int J Obes 1983; 7: 415–21.
Wright RA, Krinsky S, Fleeman C, Trujillo J, Teague E. Gastric emptying and obesity. Gastroenterology 1983; 84: 747–51.
Dubois A. Obesity and gastric emptying (Editorial). Gastroenterology 1983; 84: 875–6.
Christian PE, Datz FL, Moore JG. Gastric emptying studies in the morbidly obese before and after gastroplasty. J Nucl Med 1986; 27: 1686–90.
Maddox A, Horowitz M, Wishart J, Collins P. Gastric and oesophageal emptying in obesity. Scand J Gastroenterol 1989; 24: 593–8.
Schedl HP. Use of polyethylene glycol and phenol red as unabsorbed indicators for intestinal absorption studies in man. Gut 1966; 7: 159–63.
Bloom DS, Jacobson ED, Grossman MI. Validation of dilution indicators in the stomach. Gastroenterology 1967; 52: 205–10.
Scarr M, Maltby JR, Jani K, Sutherland LR. Volume and acidity of residual gastric fluid after oral fluid ingestion before elective ambulatory surgery. CMAJ 1989; 141: 1151–4.
Guyton AE, Hall JE. Textbook of Medical Physiology, 10th ed. Philadelphia: WB Saunders Company; 2000: 728–33.
Lind JF, Warrian WG, Wankling WJ. Responses of the gastroesophageal junctional zone to increases in abdominal pressure. Can J Surg 1966; 9: 32–8.
Jones MJ, Mitchell RW, Hindocha N. Effect of increased intra-abdominal pressure during laparoscopy on the lower esophageal sphincter. Anesth Analg 1989; 68: 63–5.
O’Mullane EJ. Vomiting and regurgitation during anaesthesia. Lancet 1954; 1: 1209–12.
Plourde G, Hardy JF. Aspiration pneumonia: assessing the risk of regurgitation in the cat. Can Anaesth Soc J 1986; 33: 345–8.
Hartsilver EL, Vanner RG, Bewley J, Clayton T. Gastric pressure during emergency caesarean section under general anaesthesia. Br J Anaesth 1999; 82: 752–4.
Roberts RB, Shirley MA. Reducing the risk of acid aspiration during cesarean section. Anesth Analg 1974; 53: 859–68.
Roberts RB, Shirley MA. Antacid therapy in obstetrics (Letter). Anesthesiology 1980; 53: 83.
Manchikanti L, Colliver JA, Marrero TC, Roush JR. Assessment of age-related acid aspiration risk factors in pediatric, adult, and geriatric patients. Anesth Analg 1985; 64: 11–7.
Sutherland AD, Stock JG, Davies JM. Effects of preoperative fasting on morbidity and gastric contents in patients undergoing day-stay surgery. Br J Anaesth 1986; 58: 876–8.
Lam AM, Grace DM, Manninen PH. The effects of cimetidine and ranitidine with and without metoclopramide on gastric volume and pH in morbidly obese patients. Can Anaesth Soc J 1986; 33: 773–9.
Schreiner MS. Gastric fluid volume: is it really a risk factor for pulmonary aspiration? Anesth Analg 1998; 87: 754–6.
Marchand P. A study on the forces productive of gastroesophageal regurgitation and herniation through the diaphragmtic hiatus. Thorax 1957; 12: 189–202.
Illing L, Duncan PG, Yip R. Gastroesophageal reflux during anaesthesia. Can J Anaesth 1992; 39: 466–70.
Hardy JF, Lepage Y, Bonneville-Chouinard N. Occurrence of gastroesophageal reflux does not correlate with the volume of gastric contents. Can J Anaesth 1990; 37: 502–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maltby, J.R., Pytka, S., Watson, N.C. et al. Drinking 300 mL of clear fluid two hours before surgery has no effect on gastric fluid volume and pH in fasting and non-fasting obese patients. Can J Anesth 51, 111–115 (2004). https://doi.org/10.1007/BF03018767
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018767